“Inflame” redirects here. For the 2017 Turkish film, see
Inflame (film).
Inflammation (from Latin inflammatio) is part of the complex biological response of body tissues to harmful stimuli, such as pathogens, damaged cells, or irritants,[1]and is a protective response involving immune cells, blood vessels, and molecular mediators. The function of inflammation is to eliminate the initial cause of cell injury, clear out necrotic cells and tissues damaged from the original insult and the inflammatory process, and to initiate tissue repair.
The classical signs of inflammation are heat, pain, redness, swelling, and loss of function. Inflammation is a generic response, and therefore it is considered as a mechanism of innate immunity, as compared to adaptive immunity, which is specific for each pathogen.[2] Too little inflammation could lead to progressive tissue destruction by the harmful stimulus (e.g. bacteria) and compromise the survival of the organism. In contrast, chronic inflammation may lead to a host of diseases, such as hay fever, periodontitis, atherosclerosis, rheumatoid arthritis, and even cancer (e.g., gallbladder carcinoma). Inflammation is therefore normally closely regulated by the body.
Inflammation can be classified as either acute or chronic. Acute inflammation is the initial response of the body to harmful stimuli and is achieved by the increased movement of plasma and leukocytes (especially granulocytes) from the blood into the injured tissues. A series of biochemical events propagates and matures the inflammatory response, involving the local vascular system, the immune system, and various cells within the injured tissue. Prolonged inflammation, known as chronic inflammation, leads to a progressive shift in the type of cells present at the site of inflammation, such as mononuclear cells, and is characterized by simultaneous destruction and healing of the tissue from the inflammatory process.
Inflammation is not a synonym for infection. Infection describes the interaction between the action of microbial invasion and the reaction of the body’s inflammatory response — the two components are considered together when discussing an infection, and the word is used to imply a microbial invasive cause for the observed inflammatory reaction. Inflammation on the other hand describes purely the body’s immunovascular response, whatever the cause may be. But because of how often the two are correlated, words ending in the suffix -itis (which refers to inflammation) are sometimes informally described as referring to infection. For example, the word urethritis strictly means only “urethral inflammation”, but clinical health care providers usually discuss urethritis as a urethral infection because urethral microbial invasion is the most common cause of urethritis.
It is useful to differentiate inflammation and infection as there are many pathological situations where inflammation is not driven by microbial invasion – for example, atherosclerosis, type III hypersensitivity, trauma, ischaemia. There are also pathological situations where microbial invasion does not result in classic inflammatory response—for example, parasitosis, eosinophilia.
Causes
Physical:
Biological:
Chemical:[3]
Psychological:
Types
Comparison between acute and chronic inflammation:
|
Acute |
Chronic |
| Causative agent |
Bacterial pathogens, injured tissues |
Persistent acute inflammation due to non-degradable pathogens, viral infection, persistent foreign bodies, or autoimmune reactions |
| Major cells involved |
neutrophils (primarily), basophils (inflammatory response), and eosinophils (response to helminth worms and parasites), mononuclear cells (monocytes, macrophages) |
Mononuclear cells (monocytes, macrophages, lymphocytes, plasma cells), fibroblasts |
| Primary mediators |
Vasoactive amines, eicosanoids |
IFN-γ and other cytokines, growth factors, reactive oxygen species, hydrolytic enzymes |
| Onset |
Immediate |
Delayed |
| Duration |
Few days |
Up to many months, or years |
| Outcomes |
Resolution, abscess formation, chronic inflammation |
Tissue destruction, fibrosis, necrosis |
Cardinal signs
The classic signs and symptoms of acute inflammation:
| English |
Latin |
| Redness |
Rubor* |
| Swelling |
Tumor* |
| Heat |
Calor* |
| Pain |
Dolor* |
| Loss of function |
Functio laesa** |
| All the above signs may be observed in specific instances, but no single sign must, as a matter of course, be present.[5]These are the original, or “cardinal signs” of inflammation.[5]*
Functio laesa is an apocryphal notion, as it is not unique to inflammation and is a characteristic of many disease states.[6]** |

Infected ingrown toenail showing the characteristic redness and swelling associated with acute inflammation
Acute inflammation is a short-term process, usually appearing within a few minutes or hours and begins to cease upon the removal of the injurious stimulus.[7] It involves a coordinated and systemic mobilisation response locally of various immune, endocrine and neurological mediators of acute inflammation. In a normal healthy response, it becomes activated, clears the pathogen and begins a repair process and then ceases.[8] It is characterized by five cardinal signs:[9]
An acronym that may be used to remember the key symptoms is “PRISH”, for pain, redness, immobility (loss of function), swelling and heat.
The traditional names for signs of inflammation come from Latin:
The first four (classical signs) were described by Celsus (ca. 30 BC–38 AD),[11] while loss of function was added later by Galen[12] even though the attribution is disputed and the origination of the fifth sign has also been ascribed to Thomas Sydenham[13] and Virchow.[7][9]
Redness and heat are due to increased blood flow at body core temperature to the inflamed site; swelling is caused by accumulation of fluid; pain is due to the release of chemicals such as bradykinin and histamine that stimulate nerve endings. Loss of function has multiple causes.[9]
Acute inflammation of the lung (usually caused in response to pneumonia) does not cause pain unless the inflammation involves the parietal pleura, which does have pain-sensitive nerve endings.[9]
Process of acute inflammation
The process of acute inflammation is initiated by resident immune cells already present in the involved tissue, mainly resident macrophages, dendritic cells, histiocytes, Kupffer cells and mast cells. These cells possess surface receptors known as pattern recognition receptors (PRRs), which recognize (i.e., bind) two subclasses of molecules: pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs). PAMPs are compounds that are associated with various pathogens, but which are distinguishable from host molecules. DAMPs are compounds that are associated with host-related injury and cell damage.
At the onset of an infection, burn, or other injuries, these cells undergo activation (one of the PRRs recognize a PAMP or DAMP) and release inflammatory mediators responsible for the clinical signs of inflammation. Vasodilation and its resulting increased blood flow causes the redness (rubor) and increased heat (calor). Increased permeability of the blood vessels results in an exudation (leakage) of plasma proteins and fluid into the tissue (edema), which manifests itself as swelling (tumor). Some of the released mediators such as bradykinin increase the sensitivity to pain (hyperalgesia, dolor). The mediator molecules also alter the blood vessels to permit the migration of leukocytes, mainly neutrophils and macrophages, outside of the blood vessels (extravasation) into the tissue. The neutrophils migrate along a chemotactic gradient created by the local cells to reach the site of injury.[7] The loss of function (functio laesa) is probably the result of a neurological reflex in response to pain.
In addition to cell-derived mediators, several acellular biochemical cascade systems consisting of preformed plasma proteins act in parallel to initiate and propagate the inflammatory response. These include the complement system activated by bacteria and the coagulation and fibrinolysis systems activated by necrosis, e.g. a burn or a trauma.[7]
The acute inflammatory response requires constant stimulation to be sustained. Inflammatory mediators are short-lived and are quickly degraded in the tissue. Hence, acute inflammation begins to cease once the stimulus has been removed.[7]
Vascular component
Vasodilation and increased permeability
As defined, acute inflammation is an immunovascular response to an inflammatory stimulus. This means acute inflammation can be broadly divided into a vascular phase that occurs first, followed by a cellular phase involving immune cells (more specifically myeloid granulocytes in the acute setting). The vascular component of acute inflammation involves the movement of plasma fluid, containing important proteins such as fibrin and immunoglobulins (antibodies), into inflamed tissue.
Upon contact with PAMPs, tissue macrophages and mastocytes release vasoactive amines such as histamine and serotonin, as well as eicosanoids such as prostaglandin E2 and leukotriene B4 to remodel the local vasculature. Macrophages and endothelial cells release nitric oxide. These mediators vasodilate and permeabilize the blood vessels, which results in the net distribution of blood plasma from the vessel into the tissue space. The increased collection of fluid into the tissue causes it to swell (edema). This exuded tissue fluid contain various antimicrobial mediators from the plasma such as complement, lysozyme, antibodies, which can immediately deal damage to microbes, and opsonise the microbes in preparation for the cellular phase. If the inflammatory stimulus is a lacerating wound, exuded platelets, coagulants, plasmin and kinins can clot the wounded area and provide haemostasis in the first instance. These clotting mediators also provide a structural staging framework at the inflammatory tissue site in the form of a fibrin lattice – as would construction scaffolding at a construction site – for the purpose of aiding phagocytic debridement and wound repair later on. Some of the exuded tissue fluid is also funnelled by lymphatics to the regional lymph nodes, flushing bacteria along to start the recognition and attack phase of the adaptive immune system.
Acute inflammation is characterized by marked vascular changes, including vasodilation, increased permeability and increased blood flow, which are induced by the actions of various inflammatory mediators. Vasodilation occurs first at the arteriole level, progressing to the capillary level, and brings about a net increase in the amount of blood present, causing the redness and heat of inflammation. Increased permeability of the vessels results in the movement of plasma into the tissues, with resultant stasis due to the increase in the concentration of the cells within blood – a condition characterized by enlarged vessels packed with cells. Stasis allows leukocytes to marginate (move) along the endothelium, a process critical to their recruitment into the tissues. Normal flowing blood prevents this, as the shearing force along the periphery of the vessels moves cells in the blood into the middle of the vessel.
Plasma cascade systems
- The complement system, when activated, creates a cascade of chemical reactions that promotes opsonization, chemotaxis, and agglutination, and produces the MAC.
- The kinin system generates proteins capable of sustaining vasodilation and other physical inflammatory effects.
- The coagulation system or clotting cascade, which forms a protective protein mesh over sites of injury.
- The fibrinolysis system, which acts in opposition to the coagulation system, to counterbalance clotting and generate several other inflammatory mediators.
Plasma-derived mediators
* non-exhaustive list
| Name |
Produced by |
Description |
| Bradykinin |
Kinin system |
A vasoactive protein that is able to induce vasodilation, increase vascular permeability, cause smooth muscle contraction, and induce pain. |
| C3 |
Complement system |
Cleaves to produce C3a and C3b. C3a stimulates histamine release by mast cells, thereby producing vasodilation. C3b is able to bind to bacterial cell walls and act as an opsonin, which marks the invader as a target for phagocytosis. |
| C5a |
Complement system |
Stimulates histamine release by mast cells, thereby producing vasodilation. It is also able to act as a chemoattractant to direct cells via chemotaxis to the site of inflammation. |
| Factor XII (Hageman Factor) |
Liver |
A protein that circulates inactively, until activated by collagen, platelets, or exposed basement membranes via conformational change. When activated, it in turn is able to activate three plasma systems involved in inflammation: the kinin system, fibrinolysis system, and coagulation system. |
| Membrane attack complex |
Complement system |
A complex of the complement proteins C5b, C6, C7, C8, and multiple units of C9. The combination and activation of this range of complement proteins forms the membrane attack complex, which is able to insert into bacterial cell walls and causes cell lysis with ensuing bacterial death. |
| Plasmin |
Fibrinolysis system |
Able to break down fibrin clots, cleave complement protein C3, and activate Factor XII. |
| Thrombin |
Coagulation system |
Cleaves the soluble plasma protein fibrinogen to produce insoluble fibrin, which aggregates to form a blood clot. Thrombin can also bind to cells via the PAR1 receptor to trigger several other inflammatory responses, such as production of chemokines and nitric oxide. |
Cellular component
The cellular component involves leukocytes, which normally reside in blood and must move into the inflamed tissue via extravasation to aid in inflammation. Some act as phagocytes, ingesting bacteria, viruses, and cellular debris. Others release enzymatic granules that damage pathogenic invaders. Leukocytes also release inflammatory mediators that develop and maintain the inflammatory response. In general, acute inflammation is mediated by granulocytes, whereas chronic inflammation is mediated by mononuclear cells such as monocytes and lymphocytes.

Neutrophils migrate from blood vessels to the infected tissue via chemotaxis, where they remove pathogens through phagocytosis and degranulation
Various leukocytes, particularly neutrophils, are critically involved in the initiation and maintenance of inflammation. These cells must be able to move to the site of injury from their usual location in the blood, therefore mechanisms exist to recruit and direct leukocytes to the appropriate place. The process of leukocyte movement from the blood to the tissues through the blood vessels is known as extravasation, and can be broadly divided up into a number of steps:
- Leukocyte margination and endothelial adhesion: The white blood cells within the vessels which are generally centrally located move peripherally towards the walls of the vessels.[14] Activated macrophages in the tissue release cytokines such as IL-1 and TNFα, which bind to their respective G protein-coupled receptors on the endothelial wall. Signal transduction induces the immediate expression of P-selectin on endothelial cell surfaces. This receptor binds weakly to carbohydrate ligands on the surface of leukocytes and causes them to “roll” along the endothelial surface as bonds are made and broken. Cytokines from injured cells induce the expression of E-selectin on endothelial cells, which functions similarly to P-selectin. Cytokines also induce the expression of integrin ligands such as ICAM-1 and VCAM-1 on endothelial cells, which mediate the adhesion and further slow leukocytes down. These weakly bound leukocytes are free to detach if not activated by chemokines produced in injured tissue. Activation increases the affinity of bound integrin receptors for ICAM-1 and VCAM-1 on the endothelial cell surface, firmly binding the leukocytes to the endothelium.
- Migration across the endothelium, known as transmigration, via the process of diapedesis: Chemokine gradients stimulate the adhered leukocytes to move between adjacent endothelial cells. The endothelial cells retract and the leukocytes pass through the basement membrane into the surrounding tissue using adhesion molecules such as ICAM-1.[14]
- Movement of leukocytes within the tissue via chemotaxis: Leukocytes reaching the tissue interstitium bind to extracellular matrix proteins via expressed integrins and CD44 to prevent them from leaving the site. A variety of molecules behave as chemoattractants, for example, C3a or C5, and cause the leukocytes to move along a chemotactic gradient towards the source of inflammation.
Phagocytosis
Extravasated neutrophils in the cellular phase come into contact with microbes at the inflamed tissue. Phagocytes express cell-surface endocytic pattern recognition receptors (PRRs) that have affinity and efficacy against non-specific microbe-associated molecular patterns (PAMPs). Most PAMPs that bind to endocytic PRRs and initiate phagocytosis are cell wall components, including complex carbohydrates such as mannans and β-glucans, lipopolysaccharides (LPS), peptidoglycans, and surface proteins. Endocytic PRRs on phagocytes reflect these molecular patterns, with C-type lectin receptors binding to mannans and β-glucans, and scavenger receptors binding to LPS.
Upon endocytic PRR binding, actin–myosin cytoskeletal rearrangement adjacent to the plasma membrane occurs in a way that endocytoses the plasma membrane containing the PRR-PAMP complex, and the microbe. Phosphatidylinositol and Vps34–Vps15–Beclin1 signalling pathways have been implicated to traffic the endocytosed phagosome to intracellular lysosomes, where fusion of the phagosome and the lysosome produces a phagolysosome. The reactive oxygen species, superoxides and hypochlorite bleach within the phagolysosomes then kill microbes inside the phagocyte.
Phagocytic efficacy can be enhanced by opsonization. Plasma derived complement C3b and antibodies that exude into the inflamed tissue during the vascular phase bind to and coat the microbial antigens. As well as endocytic PRRs, phagocytes also express opsonin receptors Fc receptor and complement receptor 1 (CR1), which bind to antibodies and C3b, respectively. The co-stimulation of endocytic PRR and opsonin receptor increases the efficacy of the phagocytic process, enhancing the lysosomal elimination of the infective agent.
Cell-derived mediators
* non-exhaustive list
| Name |
Type |
Source |
Description |
| Lysosome granules |
Enzymes |
Granulocytes |
These cells contain a large variety of enzymes that perform a number of functions. Granules can be classified as either specific or azurophilic depending upon the contents, and are able to break down a number of substances, some of which may be plasma-derived proteins that allow these enzymes to act as inflammatory mediators. |
| Histamine |
Monoamine |
Mast cells and basophils |
Stored in preformed granules, histamine is released in response to a number of stimuli. It causes arteriole dilation, increased venous permeability, and a wide variety of organ-specific effects. |
| IFN-γ |
Cytokine |
T-cells, NK cells |
Antiviral, immunoregulatory, and anti-tumour properties. This interferon was originally called macrophage-activating factor, and is especially important in the maintenance of chronic inflammation. |
| IL-8 |
Chemokine |
Primarily macrophages |
Activation and chemoattraction of neutrophils, with a weak effect on monocytes and eosinophils. |
| Leukotriene B4 |
Eicosanoid |
Leukocytes, cancer cells |
Able to mediate leukocyte adhesion and activation, allowing them to bind to the endothelium and migrate across it. In neutrophils, it is also a potent chemoattractant, and is able to induce the formation of reactive oxygen species and the release of lysosomal enzymes by these cells. |
| LTC4, LTD4 |
Eicosanoid |
eosinophils, mast cells, macrophages |
These three Cysteine-containing leukotrienes contract lung airways, increase micro-vascular permeability, stimulate mucus secretion, and promote eosinophil-based inflammation in the lung, skin, nose, eye, and other tissues. |
| 5-oxo-eicosatetraenoic acid |
Eicosanoid |
leukocytes, cancer cells |
Potent stimulator of neutrophil chemotaxis, lysosome enzyme release, and reactive oxygen species formation; monocyte chemotaxis; and with even greater potency eosinophil chemotaxis, lysosome enzyme release, and reactive oxygen species formation. |
| 5-HETE |
Eicosanoid |
Leukocytes |
Metabolic precursor to 5-Oxo-eicosatetraenoic acid, it is a less potent stimulator of neutrophil chemotaxis, lysosome enzyme release, and reactive oxygen species formation; monocyte chemotaxis; and eosinophil chemotaxis, lysosome enzyme release, and reactive oxygen species formation. |
| Prostaglandins |
Eicosanoid |
Mast cells |
A group of lipids that can cause vasodilation, fever, and pain. |
| Nitric oxide |
Soluble gas |
Macrophages, endothelial cells, some neurons |
Potent vasodilator, relaxes smooth muscle, reduces platelet aggregation, aids in leukocyte recruitment, direct antimicrobial activity in high concentrations. |
| TNF-α and IL-1 |
Cytokines |
Primarily macrophages |
Both affect a wide variety of cells to induce many similar inflammatory reactions: fever, production of cytokines, endothelial gene regulation, chemotaxis, leukocyte adherence, activation of fibroblasts. Responsible for the systemic effects of inflammation, such as loss of appetite and increased heart rate. TNF-α inhibits osteoblast differentiation. |
Morphologic patterns
Specific patterns of acute and chronic inflammation are seen during particular situations that arise in the body, such as when inflammation occurs on an epithelial surface, or pyogenic bacteria are involved.
- Granulomatous inflammation: Characterised by the formation of granulomas, they are the result of a limited but diverse number of diseases, which include among others tuberculosis, leprosy, sarcoidosis, and syphilis.
- Fibrinous inflammation: Inflammation resulting in a large increase in vascular permeability allows fibrin to pass through the blood vessels. If an appropriate procoagulative stimulus is present, such as cancer cells,[7] a fibrinous exudate is deposited. This is commonly seen in serous cavities, where the conversion of fibrinous exudate into a scar can occur between serous membranes, limiting their function. The deposit sometimes forms a pseudomembrane sheet. During inflammation of the intestine (Pseudomembranous colitis), pseudomembranous tubes can be formed.
- Purulent inflammation: Inflammation resulting in large amount of pus, which consists of neutrophils, dead cells, and fluid. Infection by pyogenic bacteria such as staphylococci is characteristic of this kind of inflammation. Large, localised collections of pus enclosed by surrounding tissues are called abscesses.
- Serous inflammation: Characterised by the copious effusion of non-viscous serous fluid, commonly produced by mesothelial cells of serous membranes, but may be derived from blood plasma. Skin blisters exemplify this pattern of inflammation.
- Ulcerative inflammation: Inflammation occurring near an epithelium can result in the necrotic loss of tissue from the surface, exposing lower layers. The subsequent excavation in the epithelium is known as an ulcer.
Inflammatory disorders
Inflammatory abnormalities are a large group of disorders that underlie a vast variety of human diseases. The immune system is often involved with inflammatory disorders, demonstrated in both allergic reactions and some myopathies, with many immune system disorders resulting in abnormal inflammation. Non-immune diseases with causal origins in inflammatory processes include cancer, atherosclerosis, and ischaemic heart disease.[7]
A large variety of proteins are involved in inflammation, and any one of them is open to a genetic mutation which impairs or otherwise dysregulates the normal function and expression of that protein.
Examples of disorders associated with inflammation include:
Atherosclerosis
Atherosclerosis, formerly considered a bland lipid storage disease, actually involves an ongoing inflammatory response. Recent advances in basic science have established a fundamental role for inflammation in mediating all stages of this disease from initiation through progression and, ultimately, the thrombotic complications of atherosclerosis. These new findings provide important links between risk factors and the mechanisms of atherogenesis. Clinical studies have shown that this emerging biology of inflammation in atherosclerosis applies directly to human patients. Elevation in markers of inflammation predicts outcomes of patients with acute coronary syndromes, independently of myocardial damage. In addition, low-grade chronic inflammation, as indicated by levels of the inflammatory marker C-reactive protein, prospectively defines risk of atherosclerotic complications, thus adding to prognostic information provided by traditional risk factors. Moreover, certain treatments that reduce coronary risk also limit inflammation. In the case of lipid lowering with statins, this anti-inflammatory effect does not appear to correlate with reduction in low-density lipoprotein levels. These new insights into inflammation in atherosclerosis not only increase our understanding of this disease but also have practical clinical applications in risk stratification and targeting of therapy for this scourge of growing worldwide importance.[15]
Allergies
An allergic reaction, formally known as type 1 hypersensitivity, is the result of an inappropriate immune response triggering inflammation, vasodilation, and nerve irritation. A common example is hay fever, which is caused by a hypersensitive response by mast cells to allergens. Pre-sensitised mast cells respond by degranulating, releasing vasoactive chemicals such as histamine. These chemicals propagate an excessive inflammatory response characterised by blood vessel dilation, production of pro-inflammatory molecules, cytokine release, and recruitment of leukocytes.[7] Severe inflammatory response may mature into a systemic response known as anaphylaxis.
Other hypersensitivity reactions (type 2 and type 3) are mediated by antibody reactions and induce inflammation by attracting leukocytes that damage surrounding tissue.[7]
Myopathies
Inflammatory myopathies are caused by the immune system inappropriately attacking components of muscle, leading to signs of muscle inflammation. They may occur in conjunction with other immune disorders, such as systemic sclerosis, and include dermatomyositis, polymyositis, and inclusion body myositis.[7]
Leukocyte defects
Due to the central role of leukocytes in the development and propagation of inflammation, defects in leukocyte functionality often result in a decreased capacity for inflammatory defense with subsequent vulnerability to infection.[7] Dysfunctional leukocytes may be unable to correctly bind to blood vessels due to surface receptor mutations, digest bacteria (Chédiak–Higashi syndrome), or produce microbicides (chronic granulomatous disease). In addition, diseases affecting the bone marrow may result in abnormal or few leukocytes.
Pharmacological
Certain drugs or exogenous chemical compounds are known to affect inflammation. Vitamin A deficiency causes an increase in inflammatory responses,[16] and anti-inflammatory drugs work specifically by inhibiting the enzymes that produce inflammatory eicosanoids. Certain illicit drugs such as cocaine and ecstasy may exert some of their detrimental effects by activating transcription factors intimately involved with inflammation (e.g. NF-κB).[17][18]
Cancer
Inflammation orchestrates the microenvironment around tumours, contributing to proliferation, survival and migration.[19] Cancer cells use selectins, chemokines and their receptors for invasion, migration and metastasis.[20] On the other hand, many cells of the immune system contribute to cancer immunology, suppressing cancer.[21] Molecular intersection between receptors of steroid hormones, which have important effects on cellular development, and transcription factors that play key roles in inflammation, such as NF-κB, may mediate some of the most critical effects of inflammatory stimuli on cancer cells.[22] This capacity of a mediator of inflammation to influence the effects of steroid hormones in cells, is very likely to affect carcinogenesis on the one hand; on the other hand, due to the modular nature of many steroid hormone receptors, this interaction may offer ways to interfere with cancer progression, through targeting of a specific protein domain in a specific cell type. Such an approach may limit side effects that are unrelated to the tumor of interest, and may help preserve vital homeostatic functions and developmental processes in the organism.
According to a review of 2009, recent data suggests that cancer-related inflammation (CRI) may lead to accumulation of random genetic alterations in cancer cells.[23]
HIV and AIDS
It has long been recognized that infection with HIV is characterized not only by development of profound immunodeficiency but also by sustained inflammation and immune activation.[24][25][26] A substantial body of evidence implicates chronic inflammation as a critical driver of immune dysfunction, premature appearance of aging-related diseases, and immune deficiency.[24][27] Many now regard HIV infection not only as an evolving virus-induced immunodeficiency but also as chronic inflammatory disease.[28] Even after the introduction of effective antiretroviral therapy (ART) and effective suppression of viremia in HIV-infected individuals, chronic inflammation persists. Animal studies also support the relationship between immune activation and progressive cellular immune deficiency: SIVsm infection of its natural nonhuman primate hosts, the sooty mangabey, causes high-level viral replication but limited evidence of disease.[29][30] This lack of pathogenicity is accompanied by a lack of inflammation, immune activation and cellular proliferation. In sharp contrast, experimental SIVsm infection of rhesus macaque produces immune activation and AIDS-like disease with many parallels to human HIV infection.[31]
Delineating how CD4 T cells are depleted and how chronic inflammation and immune activation are induced lies at the heart of understanding HIV pathogenesis––one of the top priorities for HIV research by the Office of AIDS Research, National Institutes of Health. Recent studies demonstrated that caspase-1-mediated pyroptosis, a highly inflammatory form of programmed cell death, drives CD4 T-cell depletion and inflammation by HIV.[32][33][34] These are the two signature events that propel HIV disease progression to AIDS. Pyroptosis appears to create a pathogenic vicious cycle in which dying CD4 T cells and other immune cells (including macrophages and neutrophils) release inflammatory signals that recruit more cells into the infected lymphoid tissues to die. The feed-forward nature of this inflammatory response produces chronic inflammation and tissue injury.[35] Identifying pyroptosis as the predominant mechanism that causes CD4 T-cell depletion and chronic inflammation, provides novel therapeutic opportunities, namely caspase-1 which controls the pyroptotic pathway. In this regard, pyroptosis of CD4 T cells and secretion of pro-inflmammatory cytokines such as IL-1β and IL-18 can be blocked in HIV-infected human lymphoid tissues by addition of the caspase-1 inhibitor VX-765,[32] which has already proven to be safe and well tolerated in phase II human clinical trials.[36] These findings could propel development of an entirely new class of “anti-AIDS” therapies that act by targeting the host rather than the virus. Such agents would almost certainly be used in combination with ART. By promoting “tolerance” of the virus instead of suppressing its replication, VX-765 or related drugs may mimic the evolutionary solutions occurring in multiple monkey hosts (e.g. the sooty mangabey) infected with species-specific lentiviruses that have led to a lack of disease, no decline in CD4 T-cell counts, and no chronic inflammation.
Resolution of inflammation
The inflammatory response must be actively terminated when no longer needed to prevent unnecessary “bystander” damage to tissues.[7] Failure to do so results in chronic inflammation, and cellular destruction. Resolution of inflammation occurs by different mechanisms in different tissues. Mechanisms that serve to terminate inflammation include:[7][37]
| “ |
Acute inflammation normally resolves by mechanisms that have remained somewhat elusive. Emerging evidence now suggests that an active, coordinated program of resolution initiates in the first few hours after an inflammatory response begins. After entering tissues, granulocytes promote the switch of arachidonic acid–derived prostaglandins and leukotrienes to lipoxins, which initiate the termination sequence. Neutrophil recruitment thus ceases and programmed death by apoptosis is engaged. These events coincide with the biosynthesis, from omega-3 polyunsaturated fatty acids, of resolvins and protectins, which critically shorten the period of neutrophil infiltration by initiating apoptosis. As a consequence, apoptotic neutrophils undergo phagocytosis by macrophages, leading to neutrophil clearance and release of anti-inflammatory and reparative cytokines such as transforming growth factor-β1. The anti-inflammatory program ends with the departure of macrophages through the lymphatics.[48] |
” |
| — Charles Serhan |
Connection to depression
There is evidence for a link between inflammation and depression.[49] Inflammatory processes can be triggered by negative cognitions or their consequences, such as stress, violence, or deprivation. Thus, negative cognitions can cause inflammation that can, in turn, lead to depression.[50][51][dubious – discuss] In addition there is increasing evidence that inflammation can cause depression because of the increase of cytokines, setting the brain into a “sickness mode”.[52] Classical symptoms of being physically sick like lethargy show a large overlap in behaviors that characterize depression. Levels of cytokines tend to increase sharply during depressive episodes in manics and drop off during remission.[53] Furthermore, it has been shown in clinical trials that anti-inflammatory medicines taken in addition to antidepressants not only significantly improves symptoms but also increases the proportion of subjects positively responding to treatment.[54] Inflammations that lead to serious depression could be caused by common infections such as those caused by a virus, bacteria or even parasites.[55]
Systemic effects
An infectious organism can escape the confines of the immediate tissue via the circulatory system or lymphatic system, where it may spread to other parts of the body. If an organism is not contained by the actions of acute inflammation it may gain access to the lymphatic system via nearby lymph vessels. An infection of the lymph vessels is known as lymphangitis, and infection of a lymph node is known as lymphadenitis. When lymph nodes cannot destroy all pathogens, the infection spreads further. A pathogen can gain access to the bloodstream through lymphatic drainage into the circulatory system.
When inflammation overwhelms the host, systemic inflammatory response syndrome is diagnosed. When it is due to infection, the term sepsis is applied, with the terms bacteremia being applied specifically for bacterial sepsis and viremia specifically to viral sepsis. Vasodilation and organ dysfunction are serious problems associated with widespread infection that may lead to septic shock and death.
Acute-phase proteins
Inflammation also induces high systemic levels of acute-phase proteins. In acute inflammation, these proteins prove beneficial; however, in chronic inflammation they can contribute to amyloidosis.[7] These proteins include C-reactive protein, serum amyloid A, and serum amyloid P, which cause a range of systemic effects including:[7]
Leukocyte numbers
Inflammation often affects the numbers of leukocytes present in the body:
- Leukocytosis is often seen during inflammation induced by infection, where it results in a large increase in the amount of leukocytes in the blood, especially immature cells. Leukocyte numbers usually increase to between 15 000 and 20 000 cells per microliter, but extreme cases can see it approach 100 000 cells per microliter.[7] Bacterial infection usually results in an increase of neutrophils, creating neutrophilia, whereas diseases such as asthma, hay fever, and parasite infestation result in an increase in eosinophils, creating eosinophilia.[7]
- Leukopenia can be induced by certain infections and diseases, including viral infection, Rickettsia infection, some protozoa, tuberculosis, and some cancers.[7]
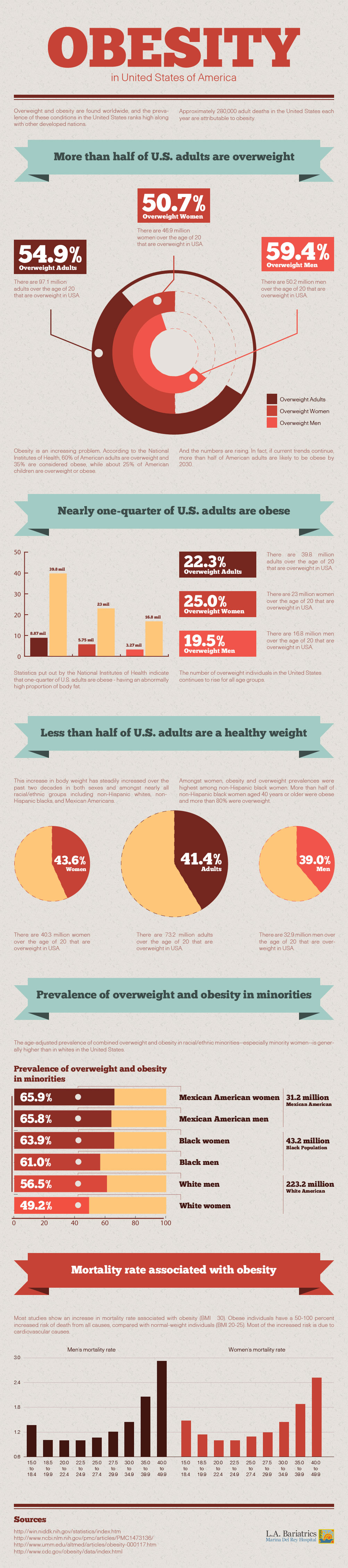
Systemic inflammation and obesity
With the discovery of interleukins (IL), the concept of systemic inflammation developed. Although the processes involved are identical to tissue inflammation, systemic inflammation is not confined to a particular tissue but involves the endothelium and other organ systems.
Chronic inflammation is widely observed in obesity.[56][57] The obese commonly have many elevated markers of inflammation, including:[58][59]
Low-grade chronic inflammation is characterized by a two- to threefold increase in the systemic concentrations of cytokines such as TNF-α, IL-6, and CRP.[62] Waist circumference correlates significantly with systemic inflammatory response.[63] A predominant factor in this correlation is due to the autoimmune response triggered by adiposity, whereby immune cells may mistake fatty deposits for intruders. The body attacks fat similar to bacteria and fungi. When expanded fat cells leak or break open, macrophages mobilize to clean up and embed into the adipose tissue. Then macrophages release inflammatory chemicals, including TNF-α and IL-6. TNF’s primary role is to regulate the immune cells and induce inflammation. White blood cells then assist by releasing more cytokines. This link between adiposity and inflammation has been shown to produce 10–35% of IL-6 in a resting individual, and this production increases with increasing adiposity.[64]
Loss of white adipose tissue reduces levels of inflammation markers.[56] The association of systemic inflammation with insulin resistance and atherosclerosis is the subject of intense research.[65]
In the obese mouse models, inflammation and macrophage-specific genes are upregulated in white adipose tissue (WAT). There were also signs of dramatic increase in circulating insulin level, adipocyte lipolysis and formation of multinucleate giant cells.[66] The fat-derived protein called angiopoietin-like protein 2 (Angptl2) elevates in fat tissues. Higher than normal Angptl2 level in fat tissues develop inflammation as well as insulin and leptin resistance. Stored fat secretes Leptin to signal satiety. Leptin resistance plays a role in the process where appetite overrules the message of satiety. Angptl2 then starts an inflammatory cascade causing blood vessels to remodel and attract macrophages. Angptl2 is an adipocyte-derived inflammatory mediator linking obesity to systemic insulin resistance.[67] It is possible that, as an inflammatory marker, leptin responds specifically to adipose-derived inflammatory cytokines.
C-reactive protein (CRP) is generated at a higher level in obese people. It raises when there is inflammation throughout the body. Mild elevation in CRP increase risk of heart attacks, strokes, high blood pressure, muscle weakness and fragility.[citation needed]
Systemic inflammation and overeating
Hyperglycemia induces IL-6 production from endothelial cells and macrophages.[68] Meals high in saturated fat, as well as meals high in calories have been associated with increases in inflammatory markers.[69][70]While the inflammatory responses are acute and arise in response to overeating, the response may become chronic if the overeating is chronic.
Bente Klarlund Pedersen wrote in 2013 that interstitial abdominal adiposity (also referred to as accumulated intra-abdominal fat) is a major and possibly primary factor in increasing systemic risk for multiple inflammatory diseases. However, she indicates that this is mediated via TNF-α, rather than Interleukin 6, which she identified as a myokine in 2003.[71] Dr. Pedersen concludes: “Until the beginning of this millennium, it was commonly thought that the increase in IL-6 during exercise was a consequence of an immune response due to local damage in the working muscles and it was hypothesized that macrophages were responsible for this increase. However, an early study demonstrated that IL-6 mRNA in monocytes did not increase as a result of exercise.”[72]
Dr. Pedersen continues (in the same article): “Patients with diabetes have a high protein expression of TNF-α in skeletal muscle and increased TNF-α levels in plasma, and it is likely that adipose tissue, which produces TNF-α, is the main source of the circulating TNF-α. In vitro studies demonstrate that TNF-α has direct inhibitory effects on insulin signaling. In addition, TNF-α infusion in healthy humans induces insulin resistance in skeletal muscle, without an effect on EGP [endogenous glucose production]. It has also been proposed that TNF-α causes insulin resistance indirectly in vivo by increasing the release of FFAs from adipose tissue. TNF-α increases lipolysis in human and 3T3-L1 adipocytes. However, TNF-α has no effect on muscle fatty acid oxidation, but increases fatty acid incorporation into diacylglycerol, which may be involved in the development of the TNF-α-induced insulin resistance in skeletal muscle. In addition, evidence suggests that TNF-α plays a direct role in linking insulin resistance to vascular disease. Moreover, in CVDs, activated immune cells also play major roles, particularly in the etiology of atherosclerosis. Importantly, also tumor initiation, promotion, and progression is stimulated by systemic elevation of proinflammatory cytokines.”[72]
Outcomes

Scars present on the skin, evidence of fibrosis and healing of a wound
The outcome in a particular circumstance will be determined by the tissue in which the injury has occurred and the injurious agent that is causing it. Here are the possible outcomes to inflammation:[7]
- Resolution
The complete restoration of the inflamed tissue back to a normal status. Inflammatory measures such as vasodilation, chemical production, and leukocyte infiltration cease, and damaged parenchymal cells regenerate. In situations where limited or short-lived inflammation has occurred this is usually the outcome.
- Fibrosis
Large amounts of tissue destruction, or damage in tissues unable to regenerate, cannot be regenerated completely by the body. Fibrous scarring occurs in these areas of damage, forming a scar composed primarily of collagen. The scar will not contain any specialized structures, such as parenchymal cells, hence functional impairment may occur.
- Abscess formation
A cavity is formed containing pus, an opaque liquid containing dead white blood cells and bacteria with general debris from destroyed cells.
- Chronic inflammation
In acute inflammation, if the injurious agent persists then chronic inflammation will ensue. This process, marked by inflammation lasting many days, months or even years, may lead to the formation of a chronic wound. Chronic inflammation is characterised by the dominating presence of macrophages in the injured tissue. These cells are powerful defensive agents of the body, but the toxins they release (including reactive oxygen species) are injurious to the organism’s own tissues as well as invading agents. As a consequence, chronic inflammation is almost always accompanied by tissue destruction.
Examples
Inflammation is usually indicated by adding the suffix “itis“, as shown below. However, some conditions such as asthma and pneumonia do not follow this convention. More examples are available at list of types of inflammation.
Diet and inflammation
The Dietary Inflammatory Index (DII) is a score (number) that describes the potential of diet to modulate systemic inflammation within the body. As stated chronic inflammation is linked to most chronic diseases including arthritis, many types of cancer, cardiovascular diseases, inflammatory bowel diseases, and diabetes.[73]
It has been known for many decades both that inflammation is linked to health and that diet is a major determinant of inflammation. Until the invention of the DII by scientists led by James R. Hébert at the Statewide South Carolina Cancer Prevention and Control Program in the University of South Carolina,[74] no indicator of diet-related inflammation had ever been devised. The DII is unique among dietary indices in that it is based on results of studies published in the peer-reviewed literature and not any of the three methods typically used to create a dietary index; i.e., Basing it on 1) a particular cuisine or foodway (e.g., the Mediterranean, Macrobiotic or South Asian diet); 2) dietary guidelines (e.g., the Healthy Eating Index, which is based on the US Dietary Guidelines); or 3) results from a particular study (which reflect biases related to sample selection, response set biases such as social desirability). By contrast, the DII: 1) is grounded in peer-reviewed literature focusing specifically on inflammation (thus obviating idiosyncrasies of specific dietary assessment methods and limitations of exposure differences within populations); 2) can be adapted to virtually any dietary assessment method capable of providing estimates of nutrient intake; and 3) has been standardized to dietary intake from representative populations around the world, thus facilitating easy quantitative comparisons across studies.
Since its invention in 2004 and the publication of a now-defunct earlier-version of the DII in December 2009,[75] the DII went through a major overhaul, resulting in a new version that replaced the old version, published first on-line in 2013 and then in hard copy in 2014.[76] This new version is superior to the earlier one in a number of ways: 1) it is based on a larger, more robust literature (see Derivation/ Computation) of 1,943 (vs. 927) articles that were reviewed and scored; 2) creation of a global dataset based on intake measures from populations in 11 countries around the world, thus allowing comparison of results from studies conducted anywhere in the world; and 3) scoring such that lower, more negative, scores indicate anti-inflammation, while higher, more positive, scores are more pro-inflammatory.[76]
This new, improved version of the DII has been subjected to construct validation, which tested (and subsequently confirmed) its ability to predict blood levels of inflammatory markers. The first of these tests showed the DII could predict repeat measures of c-reactive protein (CRP) from the Seasonal Variation of Blood Cholesterol, an intensive follow-up study of 559 adult men and women conducted in Massachusetts.[77][78] The second, based on data from 2,567 women across the USA participating in the Women’s Health Initiative Observational Study from 1993–1998, showed the DII’s ability to predict levels of interleukin (IL)-6 and tumor necrosis factor-alpha receptor-2 (TNFα-R2) and a combined inflammatory biomarker score (consisting of IL-6, TNFα-R2, and CRP).[79] Subsequently, the DII has been shown to have positive associations with IL-6 and homocysteine in the Asklepios Study in Belgium,[80][81] CRP among police officers in Buffalo, NY, USA[82] and inversely correlated with SNP rs2243250 in IL-4 among controls in the Bellvitge Colorectal Cancer Study in Spain.[83]
Derivation and computation
Briefly, based on a search of the literature from 1950 to the end of 2010, 45 food parameters were identified among foods, nutrients, and other food components that were associated with 6 plasma inflammatory markers (IL-1β, IL-4, IL-6, IL-10, TNF-α and CRP). A specific article inflammatory effect score for each food parameter on the basis of the literature review and taking into account the quality and number of published papers (1,943 articles were reviewed and scored). For each study participant in a study, the dietary data is first linked to a global database that was developed based on 11 datasets from around the world (US – NHANES; UK – The National Diet & Nutrition Survey; Bahrain – National Nutrition Survey for Adult Bahrainis; Mexico – Mexican National Health and Nutrition Survey; Australia – National Nutrition Survey; South Korea – KNHANES; Taiwan – Nutrition and Health Survey in Taiwan; India – Indian Diet Study; New Zealand – National Nutrition Survey) and thus provides a robust estimate of the mean and the standard deviation of these 45 parameters.2 Each subject’s exposure relative to the “standard global mean” is expressed as a z-score that is derived by subtracting the “standard global mean” from the amount reported, and dividing this value by its standard deviation. To minimize the effect of “right skewing”, this value was then converted to a centered percentile score. The subject’s DII score was computed by multiplying these values by the specific article inflammatory effect score for each food parameter and then summing together all these 45 values according to the following formula, DII=b1*n1+b2*n2………..b45*n45, where bi refers to the literature-derived inflammatory effect score for each of the evaluated food parameter and ni refers to the food parameter-specific centered percentile, which were derived from the dietary data, per each i from 1 to 45.[76]
Accuracy
The DII is uniquely and strongly based on empirical evidence available in the peer-reviewed literature on the relationships between dietary factors and important inflammatory markers (see Derivation/ Computation). It is important to note, however, that, as an index that superimposes on a method of dietary assessment, the DII is dependent on the accuracy of the dietary assessment method used. The DII cannot make up for deficiencies/ inaccuracies in measuring dietary intake.
Disease prevention and causation
Besides studies focusing on markers of inflammation in blood, the DII has been associated with a large number of actual health outcomes including:
- components of the metabolic syndrome, in a Spanish cohort[84] and among US police officers;[84]
- asthma and lung function in Australia;[85]
- lung cancer and other respiratory conditions in Italy;[86]
- esophageal cancer in Sweden,[87] Italy,[88] and Iran;[89]
- colorectal cancer, in two populations of US women,[90][91] Italian men and women,[92] men and women in the National Institutes of Health-American Association of Retired Persons Diet and Health Study[93] and a case-control study in Spain;[93]
- female breast cancer in Germany[94] and Sweden;[95]
- prostate cancer, in Italy[96] and Jamaica;[97]
- pancreatic cancer in Italy;[98]
- cardiovascular diseases, in the PREvencio´n con DIeta MEDiterra´nea (PREDIMED) Trial[99] and the Seguimiento Universidad de Navarra (SUN) cohort[100] in Spain, and a follow-up study of Australian men;[101]
- depression in Spain;[102]
- telomere length (an indicator of aging on a DNA level) in the Spanish PREDIMED Trial;[103]
- overall mortality in American[104] and Swedish women;[105] and
- bone mineral density in Iran.[106]
Other factors that can influence inflammation
Besides dietary factors, physical activity, fitness, sleep, shift work, and stress can affect inflammation. Also, there are auto-immune and other conditions that can influence inflammation. It has been shown that these other factors also may be related to the DII.[107]
Advantages and disadvantages of the DII
Advantages of the DII over other indices include that it: 1) focuses on a particular and very important mechanism of how dietary components affect health through inflammation; 2) is grounded in peer-reviewed literature focusing specifically on inflammatory markers known to affect health well-being; 3) can be adapted to virtually any dietary assessment method that provides estimates of nutrient intake; and 4) is standardized to dietary intake from representative populations around the world, thus facilitating easy quantitative comparisons across studies.
Disadvantages include that: 1) it is dependent on the quality of the dietary assessment upon which the computation is based (it cannot make up for deficiencies in the methods of obtaining the dietary data); and 2) it is not focused specifically on other effects of diet, though it is correlated (r (correlation coefficient) around │0.50│) with other diet indices that purport to assess diet quality.[84][103][108]
Criticism and alternatives
Criticisms include that the DII is not up to date. It must be noted that though the index was refined by the inclusion of three more years (from 2008 through 2010) of publications and more than doubling of the literature base, no major change in the overall thrust of the literature base was evident.
Exercise and inflammation
Exercise-induced acute inflammation
Acute inflammation of the muscle cells, as understood in exercise physiology,[109] can result after induced eccentric and concentric muscle training. Participation in eccentric training and conditioning, including resistance training and activities that emphasize eccentric lengthening of the muscle including downhill running on a moderate to high incline can result in considerable soreness within 24 to 48 hours, even though blood lactate levels, previously thought to cause muscle soreness, were much higher with level running. This delayed onset muscle soreness (DOMS) results from structural damage to the contractile filaments and z-disks, which has been noted especially in marathon runners whose muscle fibers revealed remarkable damage to the muscle fibers after both training and marathon competition[citation needed]. The onset and timing of this gradient damage to the muscle parallels the degree of muscle soreness experienced by the runners.
Z-disks are the point of contact for the contractile proteins. They provide structural support for transmission of force when muscle fibers are activated to shorten. However, in marathon runners and those who subscribe to the overload principle to enhance their muscles, show moderate Z-disk streaming and major disruption of thick and thin filaments in parallel groups of sarcomeres as a result of the force of eccentric actions or stretching of tightened muscle fibers.
This disruption of muscle fibers triggers white blood cells to increase following induced muscle soreness, leading to the inflammatory response observation from induced muscle soreness. Elevations in plasma enzymes, myoglobinemia, and abnormal muscle histology and ultrastructure are concluded to be associated with inflammatory response. High tension in the contractile-elastic system of muscle results in structural damage to the muscle fiber and plasmalemma and its epimysium, perimysium, and/or endomysium. The mysium damage disrupts calcium homeostasis in injured fibers and fiber bundles, resulting in necrosis that peaks about 48 hours after exercise. The products of macrophage activity and intracellular contents (such as histamines, kinins, and K+) accumulate outside cells. These substances then stimulate free nerve endings in the muscle; a process that appears accentuated by eccentric exercise, in which large forces are distributed over a relatively small cross-sectional area of the muscle[citation needed].
Post-inflammatory muscle growth and repair
There is a known relationship between inflammation and muscle growth.[110] For instance, high doses of anti-inflammatory medicines (e.g., NSAIDs) are able to blunt muscle growth.[111][112] Cold therapy has been shown to negatively affect muscle growth as well. Reducing inflammation results in decreased macrophage activity and lower levels of IGF-1[113] Acute effects of cold therapy on training adaptations show reduced satellite cell proliferation.[114] Long term effects include less muscular hypertrophy and an altered cell structure of muscle fibers.[115]
It has been further theorized that the acute localized inflammatory responses to muscular contraction during exercise, as described above, are a necessary precursor to muscle growth.[116] As a response to muscular contractions, the acute inflammatory response initiates the breakdown and removal of damaged muscle tissue.[117] Muscles can synthesize cytokines in response to contractions,[118][119][120] such that the cytokines interleukin-1 beta (IL-1β), TNF-α, and IL-6 are expressed in skeletal muscle up to 5 days after exercise.[117]
In particular, the increase in levels of IL-6 (interleukin 6), a myokine, can reach up to one hundred times that of resting levels.[120] Depending on volume, intensity, and other training factors, the IL-6 increase associated with training initiates about 4 hours after resistance training and remains elevated for up to 24 hours.[121][122][123]
These acute increases in cytokines, as a response to muscle contractions, help initiate the process of muscle repair and growth by activating satellite cells within the inflamed muscle. Satellite cells are crucial for skeletal muscle adaptation to exercise.[124] They contribute to hypertrophy by providing new myonuclei and repair damaged segments of mature myofibers for successful regeneration following injury- or exercise-induced muscle damage;[125][126][127] high-level powerlifters can have up to 100% more satellite cells than untrained controls.[128][129]
A rapid and transient localization of the IL-6 receptor and increased IL-6 expression occurs in satellite cells following contractions.[121] IL-6 has been shown to mediate hypertrophic muscle growth both in vitro and in vivo.[124] Unaccustomed exercise can increase IL-6 by up to sixfold at 5 hours post-exercise and threefold 8 days after exercise.[130] Also telling is the fact that NSAIDs can decrease satellite cell response to exercise,[111] thereby reducing exercise-induced protein synthesis.[112]
The increase in cytokines (myokines) after resistance exercise coincides with the decrease in levels of myostatin, a protein that inhibits muscle differentiation and growth.[123] The cytokine response to resistance exercise and moderate-intensity running occur differently, with the latter causing a more prolonged response, especially at the 12–24 hour mark.[123]
Developing research has demonstrated that many of the benefits of exercise are mediated through the role of skeletal muscle as an endocrine organ. That is, contracting muscles release multiple substances known as myokines, including but not limited to those cited in the above description, which promote the growth of new tissue, tissue repair, and various anti-inflammatory functions, which in turn reduce the risk of developing various inflammatory diseases. The new view that muscle is an endocrine organ is transforming our understanding of exercise physiology and with it, of the role of inflammation in adaptation to stress.[72]
Chronic inflammation and muscle loss
Both chronic and extreme inflammation are associated with disruptions of anabolic signals initiating muscle growth. Chronic inflammation has been implicated as part of the cause of the muscle loss that occurs with aging.[110][131] Increased protein levels of myostatin have been described in patients with diseases characterized by chronic low-grade inflammation.[132] Increased levels of TNF-α can suppress the AKT/mTOR pathway, a crucial pathway for regulating skeletal muscle hypertrophy,[133] thereby increasing muscle catabolism.[134][135][136] Cytokines may antagonize the anabolic effects of insulin-like growth factor 1 (IGF-1).[137][138] In the case of sepsis, an extreme whole body inflammatory state, the synthesis of both myofibrillar and sarcoplasmic proteins are inhibited, with the inhibition taking place preferentially in fast-twitch muscle fibers.[137][139] Sepsis is also able to prevent leucine from stimulating muscle protein synthesis.[118] In animal models, when inflammation is created, mTOR loses its ability to be stimulated by muscle growth.[140]
Exercise as a treatment for inflammation
Regular physical activity is reported to decrease markers of inflammation,[141][142][143] although the correlation is imperfect and seems to reveal differing results contingent upon training intensity. For instance, while baseline measurements of circulating inflammatory markers do not seem to differ greatly between healthy trained and untrained adults,[144][145] long-term training may help reduce chronic low-grade inflammation.[146]On the other hand, levels of the anti-inflammatory myokine IL-6 (interleukin 6) remained elevated longer into the recovery period following an acute bout of exercise in patients with inflammatory diseases, relative to the recovery of healthy controls.[146] It may well be that low-intensity training can reduce resting pro-inflammatory markers (CRP, IL-6), while moderate-intensity training has milder and less-established anti-inflammatory benefits.[144][147][148][149] There is a strong relationship between exhaustive exercise and chronic low-grade inflammation.[150] Marathon running may enhance IL-6 levels as much as 100 times over normal and increases total leuckocyte count and neturophil mobilization.[150]
Regarding the above, IL-6 had previously been classified as a proinflammatory cytokine. Therefore, it was first thought that the exercise-induced IL-6 response was related to muscle damage.[151] However, it has become evident that eccentric exercise is not associated with a larger increase in plasma IL-6 than exercise involving concentric “nondamaging” muscle contractions. This finding clearly demonstrates that muscle damage is not required to provoke an increase in plasma IL-6 during exercise. As a matter of fact, eccentric exercise may result in a delayed peak and a much slower decrease of plasma IL-6 during recovery.[152]
Recent work has shown that both upstream and downstream signalling pathways for IL-6 differ markedly between myocytes and macrophages. It appears that unlike IL-6 signalling in macrophages, which is dependent upon activation of the NFκB signalling pathway, intramuscular IL-6 expression is regulated by a network of signalling cascades, including the Ca2+/NFAT and glycogen/p38 MAPK pathways. Thus, when IL-6 is signalling in monocytes or macrophages, it creates a pro-inflammatory response, whereas IL-6 activation and signalling in muscle is totally independent of a preceding TNF-response or NFκB activation, and is anti-inflammatory.[153]
Several studies show that markers of inflammation are reduced following longer-term behavioural changes involving both reduced energy intake and a regular program of increased physical activity, and that, in particular, IL-6 was miscast as an inflammatory marker. For example, the anti-inflammatory effects of IL-6 have been demonstrated by IL-6 stimulating the production of the classical anti-inflammatory cytokines IL-1ra and IL-10.[153] As such, individuals pursuing exercise as a means to treat the causal factors underlying chronic inflammation are pursuing a course of action strongly supported by current research, as an inactive lifestyle is strongly associated with the development and progression of multiple inflammatory diseases. Note that cautions regarding over-exertion may apply in certain cases, as discussed above, though this concern rarely applies to the general population.
Signal-to-noise theory
Given that localized acute inflammation is a necessary component for muscle growth, and that chronic low-grade inflammation is associated with a disruption of anabolic signals initiating muscle growth, it has been theorized that a signal-to-noise model may best describe the relationship between inflammation and muscle growth.[154] By keeping the “noise” of chronic inflammation to a minimum, the localized acute inflammatory response signals a stronger anabolic response than could be achieved with higher levels of chronic inflammation.
See also
References
Anti-inflammatory
From Wikipedia, the free encyclopedia
Anti-inflammatory or antiinflammatory refers to the property of a substance or treatment that reduces inflammation or swelling. Anti-inflammatory drugs make up about half of analgesics, remedying pain by reducing inflammation as opposed to opioids, which affect the central nervous system to block pain signaling to the brain.
Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs (NSAIDs) alleviate pain by counteracting the cyclooxygenase (COX) enzyme. On its own, COX enzyme synthesizes prostaglandins, creating inflammation. In whole, the NSAIDs prevent the prostaglandins from ever being synthesized, reducing or eliminating the pain.
Some common examples of NSAIDs are aspirin, ibuprofen, and naproxen. The newer specific COX-inhibitors are not classified together with the traditional NSAIDs even though they presumably share the same mode of action.
On the other hand, there are analgesics that are commonly associated with anti-inflammatory drugs but that have no anti-inflammatory effects. An example is paracetamol (known as acetaminophen in the U.S). As opposed to NSAIDs, which reduce pain and inflammation by inhibiting COX enzymes, paracetamol has – as early as 2006 – been shown to block the reuptake of endocannabinoids,[1][2] which only reduces pain, likely explaining why it has minimal effect on inflammation; paracetamol is sometimes combined with an NSAID (in place of an opioid) in clinical practice to enhance the pain relief of the NSAID while still receiving the injury/disease modulating effect of NSAID-induced inflammation reduction (which is not received from opioid/paracetamol combinations).[3]
Side-effects
Long-term use of NSAIDs can cause gastric erosions, which can become stomach ulcers and in extreme cases can cause severe haemorrhage, resulting in death. The risk of death as a result of GI bleeding caused by the use of NSAIDs is 1 in 12,000 for adults aged 16–45.[4] The risk increases almost twentyfold for those over 75.[4] Other dangers of NSAIDs are exacerbating asthma and causing kidney damage.[4] Apart from aspirin, prescription and over-the-counter NSAIDs also increase the risk of myocardial infarction and stroke.[5]
Antileukotrines
Antileukotrines are anti-inflammatory agents which function as leukotriene-related enzyme inhibitors (arachidonate 5-lipoxygenase) or leukotriene receptor antagonists (cysteinyl leukotriene receptors) and consequently oppose the function of these inflammatory mediators. Although they are not used for analgesic benefits they are widely utilized in the treatment of diseases related to inflammation of the lungs such as asthma and COPD as well as sinus inflammation in allergic rhinitis.[6][7] They are also being investigated for use in diseases and injuries involving inflammation of the brain (ex. Parkinsons disease).[8][9]
Immune selective anti-inflammatory derivatives (ImSAIDs)
ImSAIDs are a class of peptides being developed by IMULAN BioTherapeutics, LLC, which were discovered to have diverse biological properties, including anti-inflammatory properties. ImSAIDs work by altering the activation and migration of inflammatory cells, which are immune cells responsible for amplifying the inflammatory response.[10][11] The ImSAIDs represent a new category of anti-inflammatory and are unrelated to steroid hormones or non-steroidal anti-inflammatories.
The ImSAIDs were discovered by scientists evaluating biological properties of the submandibular gland and saliva. Early work in this area demonstrated that the submandibular gland released a host of factors that regulate systemic inflammatory responses and modulate systemic immune and inflammatory reactions. It is now well accepted that the immune, nervous, and endocrine systems communicate and interact to control and modulate inflammation and tissue repair. One of the neuroendocrine pathways, when activated, results in the release of immune-regulating peptides from the submandibular gland upon neuronal stimulation from sympathetic nerves. This pathway or communication is referred to as the cervical sympathetic trunk-submandibular gland (CST-SMG) axis, a regulatory system that plays a role in the systemic control of inflammation.[12]
Early work in identifying factors that played a role in the CST-SMG axis lead to the discovery of a seven amino acid peptide, called the submandibular gland peptide-T. SGP-T was demonstrated to have biological activity and thermoregulatory properties related to endotoxin exposure.[13] SGP-T, an isolate of the submandibular gland, demonstrated its immunoregulatory properties and potential role in modulating the cervical sympathetic trunk-submandibular gland (CST-SMG) axis, and subsequently was shown to play an important role in the control of inflammation.
One SGP-T derivative is a three-amino acid sequence shown to be a potent anti-inflammatory molecule with systemic effects. This three-amino acid peptide is phenylalanine–glutamine–glycine (FEG) and its D-isomeric form (feG) have become the foundation for the ImSAID category.[14] Cellular Effects of feG: The cellular effects of the ImSAIDs are characterized in a number of publications. feG and related peptides are known to modulate leukocyte (white blood cells) activity by influencing cell surface receptors to inhibit excessive activation and tissue infiltration.
One lead ImSAID, the tripeptide FEG (Phe-Glu-Gly) and its D-isomer feG are known to alter leukocyte adhesion involving actions on αMβ2 integrin, and inhibit the binding of CD16b (FCyRIII) antibody to human neutrophils.[15] feG has also been shown to decrease circulating neutrophil and eosinophil accumulation, decrease intracellular oxidative activity, and reduce the expression of CD49d after antigen exposure.[16][17][18]
Bioactive compounds
Many bioactive compounds showed anti-inflammatory activities on albino rat. Anti-inflammatory activity of Plumbago zeylanica consists of Bioactive compound Plumbagin showed high activity in very low concentration.[19] More recently plumericin from the Amazonian plant Himatanthus sucuuba has been described as a potent anti-inflammatory agent in vitro and in vivo.[20]
Long-term effects
Anti-inflammatory treatment trials for existing Alzheimer’s disease have typically shown little to no effect on halting or reversing the disease.[21][22] Research and clinical trials continue.[23] Two studies from 2012 and 2013 found regular use of aspirin for over ten years is associated with an increase in the risk of macular degeneration.[24][25]
Ice treatment
Applying ice, or even cool water, to a tissue injury has an anti-inflammatory effect and is often suggested as an injury treatment and pain management technique for athletes. One common approach is rest, ice, compression and elevation. Cool temperatures inhibit local blood circulation, which reduces swelling in the injured tissue.
Health supplements
In addition to medical drugs, some herbs and health supplements may have anti-inflammatory qualities: bromelain from pineapples (Ananas comosus).[26] Cannabichromene, a cannabinoid, also has anti-inflammatory effect.[27] Honokiol from Magnolia inhibits platelet aggregation, and works as an inverse agonist at the CB2 receptor. Black seed (Nigella sativa) has shown anti-inflammatory effect due to its high thymoquinone content.[28] St. John’s wort‘s chief constituent, hyperforin, has been found to be a potent COX-1 and 5-LO inhibitor, with anti-inflammatory effect several fold that of aspirin.[citation needed]
Coal tar has been used for centuries for its anti-inflammatory and analgesic effects. Oral administration for central effects is now rare as coal tar also contains a range of dangerous and carcinogenic compounds, and does not allow for the administration of standardized doses, although some doctors readily utilize coal tar preparations for topical administration (ex. Denorex, Psoriasin) in the treatment of skin conditions such as eczema and atopic dermatitis. Many modern analgesics and anti-inflammatory agents (ex. paracetamol, and its previously used predecessor phenacetin) are derived from compounds which were originally discovered during studies to elucidate the chemicals responsible for the tars reputed health benefits.[29][30]
Anti-inflammatory foods
Prostaglandins are hormone-like substances that affect the body in variety of ways, also regulating inflammatory mediation. An anti-flammatory diet includes fewer foods that create inflammation-causing prostaglandins (PGE2) in the body, and more foods that create anti-inflammatory prostaglandins (PGE1 and PGE3).[31][not in citation given]
Suggested diets to reduce inflammation include those rich in vegetables and low in simple carbohydrates and fats, such as saturated fats and trans fats.[32] Anti-inflammatory foods include most colorful fruits and vegetables, oily fish (which contain higher levels of omega-3 fatty acids), nuts, seeds, and certain spices, such as ginger, garlic and cayenne. Extra-virgin olive oil contains the chemical oleocanthal that acts similarly to ibuprofen. Those following an anti-inflammatory diet will avoid refined oils and sugars, and show a preference for so-called anti-inflammatory foods in their meal choices.[33][34]
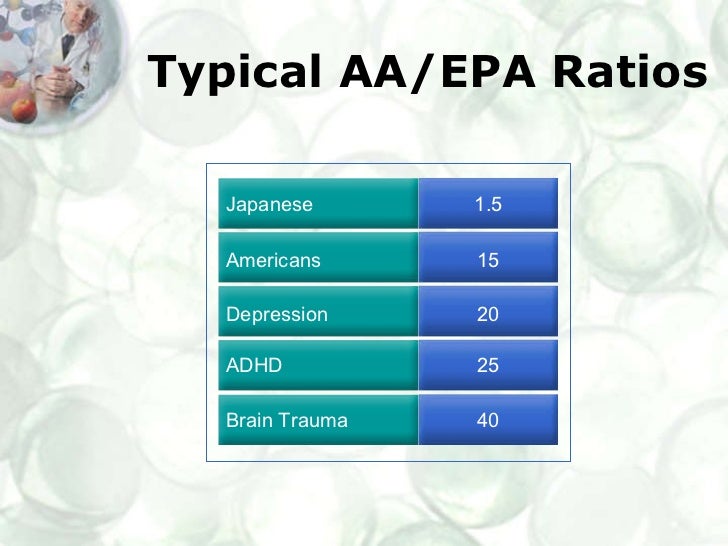
Omega-3 fatty acids have been shown to disrupt inflammation cell signaling pathways by binding to the GPR120 receptor.[35] This benefit however can be inhibited or even reversed if the ratio of Omega-6/Omega-3 is too high as Omega-6 serves as a precursor to inflammatory chemicals (prostaglandin and leukotriene eicosanoids) in the body.[36][37] A high proportion of omega-6 to omega-3 fat in the diet shifts the physiological state in the tissues toward the pathogenesis of many diseases: prothrombotic, proinflammatory and proconstrictive.[36] Omega-6 competes with Omega-3 for the same rate limiting factor which is required for the health-benefits of Omega-3, directly reducing the action of Omega-3 in addition to pharmacologically counteracting Omega-3 benefits through its own action as a pro-inflammatory agent.
Measurement of dietary inflammation
The Dietary Inflammatory Index (DII) is a score (number) that describes the potential of diet to modulate systemic inflammation within the body. Until the creation of the DII by scientists led by Dr. James R. Hébert at the Statewide South Carolina Cancer Prevention and Control Program in the University of South Carolina, no indicator of diet-related inflammation had ever been devised. The DII has been subjected to construct validation, which tested (and subsequently confirmed) its ability to predict blood levels of inflammatory markers.
Exercise
Developing research has demonstrated that many of the benefits of exercise are mediated through the role of skeletal muscle as an endocrine organ. That is, contracting muscles release multiple substances known as myokines which promote the growth of new tissue, tissue repair, and various anti-inflammatory functions, which in turn reduce the risk of developing various inflammatory diseases.[38]
Interactions with NSAIDs
Patients on NSAIDs should seek to avoid excessive consumption of Omega-6 containing foods. Although many such foods contain the anti-inflammatory Omega-3 as well, low doses of Omega-6 interfere with Omega-3’s ability to reduce inflammation, while higher doses are capable of completely inhibiting the effects of most currently-used anti-inflammatory agents (cyclooxygenase 1 inhibitors, cyclooxygenase 2 inhibitors, and antileukotrienes).[39][40][41]
The concomitant use of NSAIDs with alcohol and/or tobacco products significantly increases the already elevated risk of peptic ulcers during NSAID therapy.[42]
NSAID painkillers may interfere with and reduce the efficacy of SSRI antidepressants through inhibiting TNFα and IFNγ, both of which are cytokine derivatives.[43]
References






.png)

































.jpg)



